
Normal Pressure Hydrocephalus (NPH)
What is Normal Pressure Hydrocephalus (NPH)?
Normal pressure hydrocephalus (NPH) is when there is a build-up of cerebrospinal fluid (CSF) in an area in the center of the brain called (ventricles). This causes the ventricles to become enlarged, sometimes with little or no increase in intracranial pressure (ICP).
Who Develops Normal Pressure Hydrocephalus (NPH)?
Normal pressure hydrocephalus (NPH) is most commonly seen in adults aged 60 or over.
A recent study estimates that 800,000 older Americans may be living with NPH, and it is estimated that more than 80% of cases remain unrecognized or untreated. Without appropriate diagnostic testing, NPH is often misdiagnosed as Alzheimer’s disease or Parkinson’s disease, the result of a stroke, or other neurodegenerative conditions. Sometimes the symptoms are mistakenly attributed to “normal aging”.
NPH is, however, one of the few treatable forms of dementia. Check out our Ask the Expert Video for insights into dementia and normal pressure hydrocephalus (NPH).
What Causes Normal Pressure Hydrocephalus (NPH)?
In most cases, doctors cannot pinpoint the exact cause of normal pressure hydrocephalus (NPH). The majority of cases are referred to as idiopathic, also known as primary NPH. It means that even after thorough medical evaluation, the reasons behind the impaired circulation and absorption of CSF that lead to NPH are still unclear.
However, some people can develop NPH as a result of a known cause, which is referred to as secondary NPH. In these cases it can be the result of one of the following:
- Head injury
- Cranial surgery
- Subarachnoid hemorrhage
- Tumor or cyst
- Subdural hematomas
- Bleeding during surgery
- Meningitis and other brain infections
It is also understood that some people are born with hydrocephalus but don’t develop symptoms until late in life. They may be completely unimpaired until their hydrocephalus is detected through CT or MRI scans performed for unrelated reasons. Currently, it’s unknown what percentage of asymptomatic congenital hydrocephalus patients will eventually develop symptoms of NPH.
What are the Symptoms of Normal Pressure Hydrocephalus (NPH)?
Normal pressure hydrocephalus symptoms are typically characterized by three major indicators: gait disturbance (difficulty walking), cognitive impairment (problems with thinking), and impaired bladder control (trouble “holding it”, not able to get to the bathroom fast enough, experiencing accidents). These symptoms may not all occur simultaneously and can emerge at different stages of the disease with varying levels of severity.
Gait Disturbance (Difficult Walking):
A gait disturbance is often the most troubling symptom and can be the first to become apparent. They can range from mild imbalance to an inability to stand or walk at all. To see an example of gait disturbance, we invite you to watch the video provided below.
Characteristics of gait disturbance:
- The gait disorder is usually slow and involves, short-steps.
- Walks might appear wide-based, and shuffling.
- Trouble going down stairs or downsloping surfaces is common.
- Difficult making turns and they are often made with a series of choppy, short steps.
- People feel hesitant when approaching objects in their path
- Trouble maintaining a uniform walking pace, or sometimes a tendency to accelerate unintentionally.
- A delayed or absent protective response to balance loss contributes to an increase in falls as well as the need to reach out to walls or furniture while walking to stabilize is common.
Unique feelings and sensations:
- Some people report feeling heavy feet, as though they are magnetically attracted to the floor—a “magnetic” gait.
- Others find themselves stuck and unable to initiate a normal stride – “freezing of gait.”
Cognitive Impairments (Problems with Thinking)
Cognitive impairments, or mild dementia, are another symptom of NPH. They can involve a range of difficulties that affect daily life and thinking.
Symptoms of cognitive impairments:
- Loss of interest in daily activities
- Feeling withdrawn
- Talking less
- Mood changes
- Difficulty dealing with routine tasks
- Difficulty making decisions or multi-tasking
- Having a hard time paying attention<
- Poor handwriting
- Trouble with simple math calculations
- Forgetfulness
- Short-term memory loss.
Urinary Incontinence (Trouble Controlling the Bladder):
Urinary incontinence, or difficulty controlling the bladder, is another symptom of NPH that can affect daily life and well-being.
Types of urinary incontinence:
- In mild cases, urinary incontinence is typically characterized by urinary frequency and urgency
- In more severe cases, there can be a complete loss of bladder control, leading to unintentional leakage of urine.
Variability in symptoms:
- Some individuals with NPH experience mild urinary frequency and urgency.
- In severe cases, bladder control might be completely lost, resulting in urinary incontinence.
- Not everyone with NPH will have noticeable bladder problems; some people may never display signs of bladder problems.
Learn more about NPH by viewing a session from our National Conference on Hydrocephalus below.
How is Normal Pressure Hydrocephalus (NPH) Diagnosed?
What makes the diagnosis of normal pressure hydrocephalus (NPH) difficult is the fact that normal pressure hydrocephalus symptoms occur in other conditions that are common in an aging population, such as Parkinson’s disease (PD), osteoarthritis, peripheral neuropathy, and Alzheimer’s disease (AD).
NPH-like symptoms can occur in Alzheimer’s, vascular dementia, and Parkinson’s disease, or NPH may be a secondary condition. In NPH, not all of the symptoms arise at the same time. The combination of dementia-like symptoms, walking problems, and urinary problems (the “classic” Hakim triad – named after Salomon Hakim, MD, PhD, the clinician who first defined NPH over 50 years ago) alert healthcare providers to the possibility of NPH.
When healthcare professionals suspect possible NPH, they can help by offering a prompt referral to a neurologist or neurosurgeon.
One or more of the following tests are usually performed to confirm the diagnosis and to assess if a person is a good candidate for surgery:
- Brain imaging exam to identify enlarged ventricles
- Magnetic Resonance Imaging (MRI)
- Computed tomography (CT scans)
- Cisternography
- Neuropsychological testing
- Gait Assessment
- Lumbar CSF
Magnetic resonance imaging (MRI) is a diagnostic technique that produces images of the brain—but unlike CT scanning, MRI does not use X-rays/radiation. Instead, MRI uses radio signals and a very powerful magnet to scan the patient’s body, and the signals are then formed into pictures by a computer. MRI is a painless procedure and has no known side effects. There are two types of MRI scans:
- The Single Shot Fast Spin Echo (also called a “quick brain MRI”), which takes about three minutes and rarely requires sedation, is used to assess ventricular size.
- The full MRI, which takes 30 to 60 minutes and may require sedation, shows more minute details.
Some physicians believe that high CSF flow through the aqueduct predicts improvement with the treatment of NPH. The MRI provides more information than the CT, and is, therefore, the test of choice in most cases, but people with cardiac pacemakers or certain other metallic implants may not be able to have MRI scans because of potential interference with these devices.
Computed tomography (CT scans) is a reliable procedure for diagnosing and assisting in the management of hydrocephalus. It is a sophisticated technique in which X-ray beams are passed through a patient’s body, and pictures of the internal structures, in this case, the brain, are made by the computer.
Neuropsychological testing is the most accurate means of determining and documenting cognitive strengths and problems and can help provide a more accurate diagnosis of the range of neuropsychological and cognitive issues. The testing involves answering questions and performing tasks.
- An individual’s appearance, mood, anxiety level, and experience of delusions or hallucinations are evaluated.
- Cognitive abilities such as memory, orientation to time and place, attention, use of language, and abilities to carry out a range of tasks and follow instructions are assessed.
- Reasoning, abstract thinking, and problem-solving are analyzed.
Gait assessment performed by a licensed physical therapist is often very useful in determining the degree of impairment of an individual. It is also useful for following patients after shunt surgery or endoscopic third ventriculostomy (ETV) to evaluate the success of the surgical treatment.
Predicting shunt response:
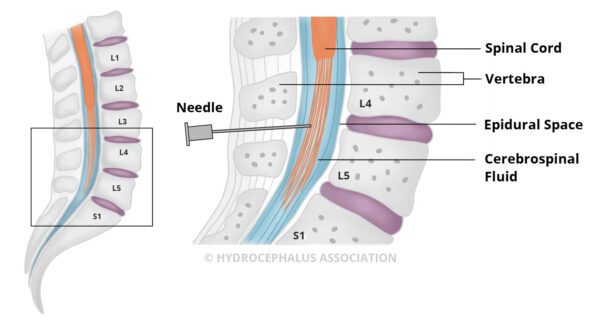
- A lumbar puncture, also known as a spinal tap, is a significant test in predicting how an individual might respond to a shunt, a common form of surgical treatment for those with NPH. Under local anesthetic, a thin needle is carefully inserted into the spinal fluid space in the lower back. Up to 50 cc of CSF is removed and doctors observe to see if one or more symptoms are temporarily relieved due to the reduced CSF volume. If symptoms are lessened or reversed by the removal of CSF, even if temporary, this suggests that surgical treatment is likely to be successful. It is helpful to have quantitative gait/cognitive testing before and after the LP to assess the significance of the degree of improvement.
A limitation of lumbar puncture and removal of a small volume of CSF as a screening test for NPH is that some people may have little or no improvement after the test, and yet may still improve with a shunt. When the response to a lumbar puncture is “negative” or uncertain, further evaluation may be helpful. - External lumbar drainage, also known as lumbar catheter insertion or continuous lumbar drainage, is a test that takes place in a hospital setting. In this procedure, a flexible tube (catheter) is carefully placed to drain CSF, which is similar to what happens during a lumbar puncture. The purpose is to imitate the effects of a shunt, a common treatment for NPH.
During the external lumbar drainage, the catheter allows for either removing spinal fluid intermittently or continuously over several days. This mimics the way a shunt affects fluid drainage and provides a more accurate measurement of CSF pressure. When drainage is intermittent, individuals are free to move around when the fluid is not being drained.
The procedure acts as a “test drive” of a shunt, helping doctors to assess potential benefits without immediately resorting to shunt surgery. However, because it involves staying in the hospital and carries some risks, it may not be recommended for all patients. People who show significant improvement with spinal fluid drainage are likely to respond to shunt surgery. Some doctors advocate using the pressure results for selecting the type of shunt or initial shunt setting for programmable and adjustable valves. - The measurement of CSF outflow resistance is a more involved test that requires a specialized clinical setting. This test begins with a lumbar tap and assesses the degree of blockage of CSF absorption back into the bloodstream. It requires the simultaneous infusion of artificial spinal fluid and the measurement of CSF pressure. If the calculated resistance value is abnormally high, then there is a very good chance that the patient will improve with shunt surgery, since the shunt mimics the function of the body’s normal CSF drainage pathways.
- For ICP monitoring or spinal pressure monitoring, a small pressure monitor is surgically inserted through the skull into the brain or ventricles or in the lumbar region to measure the intracranial pressure (ICP). Pressure monitoring, either by the lumbar catheter or the intracranial method, requires admission to a hospital. It can detect an abnormal pattern of pressure waves as well as low or high pressure. It is possible for NPH to occur even when CSF pressure is not measurably high. The results of this test can also be used to select initial shunt pressure if a shunt is being implanted.
Diagnostic tests such as those mentioned above assist medical professionals in determining the existence and severity of NPH in a patient, as well as the potential treatment options.
The presence of such potentially co-morbid diseases like Alzheimer’s and Parkinson’s can now be estimated through specialized brain scans and spinal fluid analysis. The use of these techniques can help clinicians decide if NPH should continue to be pursued, particularly if the response following a lumbar puncture or external lumbar drainage is minimal or equivocal.
How is Normal Pressure Hydrocephalus (NPH) Treated?
The most common, and typically the only available treatment for normal pressure hydrocephalus (NPH) is the surgical implantation of a shunt.
In the past five to ten years, new diagnostic techniques, better shunt design, and recognition of prognostic factors have improved patient selection and outcomes for NPH treatment. Although the insertion of a shunt is a relatively simple neurosurgical procedure that is completed in less than one hour, the decision to undergo shunt surgery is complex.
Shunt System
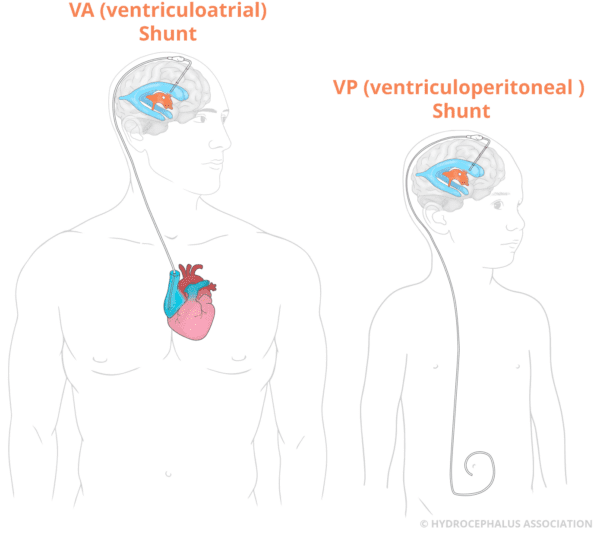
A shunt is a flexible tube placed into the ventricular system of the brain that diverts the flow of CSF into another region of the body, most often the abdominal cavity, where it can be absorbed. A valve within the shunt maintains CSF at normal levels and pressure within the ventricles.
Endoscopic Third Ventriculostomy (ETV)
A surgical procedure called endoscopic third ventriculostomy (ETV) may be considered as an alternative to a shunt for people diagnosed with aqueductal stenosis, a narrowing of the aqueduct of Sylvius located in the brain. In this procedure, the neurosurgeon uses a special endoscope to create an alternative CSF passageway that bypasses the obstruction at the cerebral aqueduct.
Determination of aqueductal stenosis can be made by MRI. The success of ETV in adults is variable, and some people who undergo the procedure later require shunt surgery to treat their symptoms. Clinical trials are currently exploring ETV as a treatment for NPH.
To find an adult neurosurgeon, visit our Physicians’ Directory.

NPH can be difficult to explain, especially to younger family members who may be confused or worried. My Hydro Bear has a shunt, offering a simple visual that helps you talk about treatment, answer questions, and make conversations feel easier and less intimidating. Many adults also find it comforting to keep as a symbol of their journey.
Management of Normal Pressure Hydrocephalus (NPH)
Normal pressure hydrocephalus (NPH) can be treated with a shunt system. However, this surgical procedure can result in complications days after the surgery or years later. The most common shunt complications are malfunction and infection as well as a subdural hematoma.
What are the signs and symptoms of a shunt malfunction or ETV closure?
Symptoms of shunt malfunction or ETV closure can vary from person to person. It’s important to be aware of what your symptoms were prior to treatment so that you or your caregiver are able to tell your physician if symptoms return. Returning symptoms may be a sign of an obstructed or malfunctioning shunt.
Symptoms of a complication in normal pressure hydrocephalus (NPH):
- Mild dementia (Forgetfulness, confusion, trouble thinking or focusing)
- Urgency to urinate or loss of bladder control
- Difficulty walking/gait disturbances
- Poor balance
- Falling
- Feeling withdrawn or talking less
- Mood changes
- Return of pre-treatment symptoms
- Signs of infection, such as fever, redness, or swelling at the shunt site
You can also explore Complications of Shunt Systems, Shunt Malfunction: Frequently Asked Questions, and Shunt Infection: Symptoms, Treatment, and Recovery to learn more.
For additional insights into the return of symptoms in NPH, please watch this video:
What is the Prognosis After Surgery?
Symptom improvement after shunt surgery to treat normal pressure hydrocephalus (NPH) is impacted by a number of variables. It’s estimated that more than 80% of those properly diagnosed with NPH and screened for shunt responsiveness will experience rapid improvement in their condition, although it may take weeks or months to see the full benefits of the procedure. The most significant improvement is seen in gait followed cognition.
Physical therapy aimed at addressing gait and balance issues plays a crucial role in facilitating a safe and independent gait, as well as fostering progress toward independent functioning within the community.
While early diagnosis often correlates with successful treatment outcomes, even patients with longstanding symptoms may experience improvement with proper treatment.
You’re not alone. The journey with NPH can be frustrating and unpredictable.
For those living with NPH and their caregivers, staying informed about the condition is essential to managing care. The challenges of living with a chronic illness or caring for a chronically ill parent or spouse are stressful for all involved. Adults with hydrocephalus may resent their dependence on a spouse, child, or another family member. Acknowledging emotional responses to this chronic and potentially disabling condition can help all those involved.
We provide essential tools and resources that enable you to have more control of your life. There is a large community across the country that is engaged and connected through the Hydrocephalus Association. We are ready to support you and your family.
There is currently a great deal of interest in the diagnosis and management of NPH, with the expectation that the reported incidence of this condition will increase dramatically as baby boomers reach retirement age and beyond. Physicians, medical device manufacturers, and patient advocates are cooperating on a variety of levels to improve methods of diagnosis, techniques and devices for treatment, and public awareness of NPH. It is anticipated that these efforts will result in years of a better quality of life for people affected by this condition.
Normal Pressure Hydrocephalus (NPH) Left Untreated
Normal pressure hydrocephalus (NPH) is typically characterized by progressive symptoms that require intervention on some level. Without treatment, normal pressure hydrocephalus symptoms may worsen and could result in death. No one is able to predict how fast the symptoms will progress, and the seriousness of symptoms may vary from day to day.
For patients whose symptoms are very mild, their doctor may advocate for close monitoring of the clinical condition without proceeding immediately to treatment with a shunt. Monitoring allows the doctor to be assured of the diagnosis as well as determine if the NPH is the primary medical condition or if there are other medical conditions occurring with the NPH. This determination will impact the treatment plan.
Some individuals with NPH may not be a candidate for treatment, despite a definitive diagnosis of NPH. Many patients that face this seek a second or third opinion from a neurosurgeon experienced in NPH. Some reasons an individual may not be a candidate include evidence from testing to remove fluid, the presence of other medical conditions, and poor health.
In this case, the doctor will continue to follow the patient closely and assist the individual and their loved ones in preparation for the progression of symptoms. This may include referrals to social work or elder care management services as well as physical therapy to assess their current functional status and adaptive equipment to assist with mobility needs and decrease the risk of falls.
2019 Ask the Expert Video Series on NPH
Dr. Mark Luciano, neurosurgeon, and Dr. Abhay Moghekar, neurologist, answer commonly asked questions from our community focused on adults living with hydrocephalus. This Ask the Expert NPH Video Series was made possible through the generosity of our industry partner Codman, a part of Integra Lifesciences who we thank for supporting this important program!
For a deeper understanding of NPH, watch our Ask the Expert: NPH Video Series
 Learn more about where the name, normal pressure hydrocephalus, originates from and Dr. Salom Hakim.
Learn more about where the name, normal pressure hydrocephalus, originates from and Dr. Salom Hakim.
The name for normal pressure hydrocephalus (NPH) originates from Dr. Salomon Hakim’s 1964 paper describing certain cases of hydrocephalus in which the group of three neurologic symptoms mentioned earlier in this article, occurred in the presence of ’normal‘ CSF pressure. These findings were observed before continuous pressure-recording techniques were available.
Information you can trust! This article was produced by the Hydrocephalus Association, copyright 2024. We would like to thank the following individuals for their valuable contributions and expert input: James B. Golomb, MD, and Sharon Hayden, PT.