
ETV-CPC for the treatment of infants with hydrocephalus
By: Dr. Jenna Koschnitzky, National Director of Research Programs
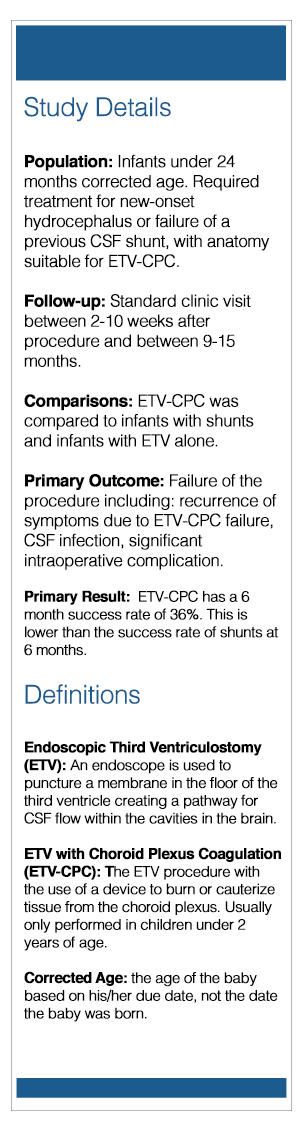
The Background
Many people have been hearing about a new procedure called Endoscopic Third Ventriculostomy with Choroid Plexus Coagulation (ETV-CPC). In Africa, the ETV-CPC has been used effectively to treat hydrocephalus and reduce the number of infants who are dependent on shunts. The pressure to reduce shunt-dependence is especially high in Africa because, once treated, many children are not able to return quickly to a neurosurgery clinic for urgent revisions. The benefit of ETV-CPC is that, if it is successful, the children are less likely to need later revisions and, unlike the ETV alone, it appears to work reasonably well in children younger than 2 years old.
In recent years, many of the neurosurgeons in the United States and Canada have gone to Africa to learn this surgical technique, including many neurosurgeons from the Hydrocephalus Clinical Research Network (HCRN). These neurosurgeons then began performing the procedure on infants at their home hospitals. However, the reasons why infants in North America develop hydrocephalus are often different from the reasons why infants in Africa develop hydrocephalus. Therefore, it was unclear if ETV-CPC provided a benefit to the infants in North America.
The Study
To determine if ETV-CPC provided a benefit compared to ETV alone or placement of a shunt, the HCRN decided to conduct a study. This study was recently published in the Journal of Neurosurgery: Pediatrics. Lead author on the study was Dr. Abhaya Kulkarni from the Hospital for Sick Children, University of Toronto.
The Results
In this study, ETV-CPC was found to be safe. The HCRN reported low rates of complications during surgery and low rates of complications after surgery.
One area of concern was the 5% rate of post-operative seizures. These primarily occurred in very young infants (less than 1 month corrected age). Overall, the ETV-CPC six month success rate was 36%. Infants who were older, had smaller ventricles, and who had more choroid plexus cauterized tended to have higher success rates.
Compared to infants who had received a shunt, the ETV-CPC had a lower six month success rate (ETV-CPC: 36% compared to Shunt: ~76%). In this study the authors matched up infants with ETV-CPC to similar infants who had received a shunt. This ensures the groups that were being compared were similar. Compared to ETV alone, the ETV-CPC had a similar success rate. However, it was more difficult to match up infants for ETV-CPC and ETV alone, so these groups were smaller and did not include many important types of hydrocephalus.
The Conclusions
This was a prospective study using high-quality data from the HCRN. ETV-CPC was shown to be safe. Infants that tended to have greater ETV-CPC success were older, had smaller ventricles, and had more choroid plexus cauterized. Six months after initial surgery, the success rate of ETV-CPC was lower than the success rate of shunts. However, there may still be significant long-term benefit of ETV-CPC for some infants.
For access to the original article please visit: https://www.ncbi.nlm.nih.gov/pubmed/29243972
The article will also be accessible on the HCRN website: https://hcrn.org/research/publications/